Key points
Question
What are the main differences in the implementation of advanced home-based care models across Ibero-American countries?
Findings
In this cross-sectional survey including senior professionals from Brazil, Colombia, Chile, Argentina, and Spain, significant inter-country differences were identified in regulation, financing, and technology (p = .015). Brazil and Colombia achieved the highest implementation scores, whereas workforce training and digital infrastructure were the weakest domains across the region.
Meaning
The findings highlight the need for coordinated regional strategies to harmonize regulatory and quality standards, enhance professional training, and strengthen digital infrastructure. Regional organizations such as ASIADES could play a key role in promoting collaboration and the sustainable advancement of home-based care in Ibero-America.
Introduction
Recent data highlights a significant growth in home-based care across Ibero-America, reflecting growing demand for care provided outside traditional healthcare settings. For example, in Spain, the percentage of long-term care recipients over 65 years old receiving care at home increased by approximately 5% between 2009 and 2019.1 In Brazil, the home care sector increased notably, with its workforce increasing by 18.87% between 2018 and 2020, the number of home care companies more than doubling between 2017 and 2022, and the number of patient beds in home care increasing in 72.3% of cities between 2019 and 2021.2
Currently, this growth is observed throughout various countries and is regulated internally within each nation.3 However, there is a limited international consensus on standards and heterogeneous regulations combined with the rapid expansion of home-based healthcare, such as: Home-Based Primary Care (HBPC) defined as the provision of primary care within the patient’s home, with a primary emphasis on the continuous management and follow-up of chronic diseases; Advanced Home Medicine (AHM) extends this concept by integrating high-complexity medical services into the home setting, encompassing remote monitoring, multidisciplinary support, and seamless continuity of care; and Hospital at Home (HaH) that constitutes a model of home hospitalization in which patients receive comprehensive medical care equivalent to that of an inpatient hospital stay, but without the necessity of physical hospital admission. This heterogeneity leads to significant differences in implementation across countries.4–6 and inconsistencies in protocols and standards may influence patient indication and access to care, potentially leading to significant disparities in care quality and clinical outcomes.7,8
Limited international cooperation can prevent countries from learning from successful models and lead to less effective practices. It also weakens the region’s ability to address common challenges. Therefore, understanding the differences and similarities in home care models across Ibero-America is essential to guide improvements toward more equitable practices. Although international collaboration is valuable, regional cooperation among Ibero-American countries is particularly relevant due to shared linguistic, cultural, and organizational features, as well as similar regulatory and financing challenges within mixed public–private health systems.
Although this paper broadly refers to home-based care, its primary focus is on advanced home care models - that is, care models that provide higher-intensity, more complex health services in the home setting, often serving as a substitute for hospital-level care.
The main objective of this study is to analyze differences in home-based care models throughout Ibero-America by evaluating national regulatory frameworks, service provision approaches, and quality assurance measures. In doing so, it aims to support international cooperation through organizations such as ASIADES (Ibero-American Association of Home Healthcare), promoting the establishment of common standards and fostering innovation, equity, and knowledge exchange.
Methods
Study design and participants
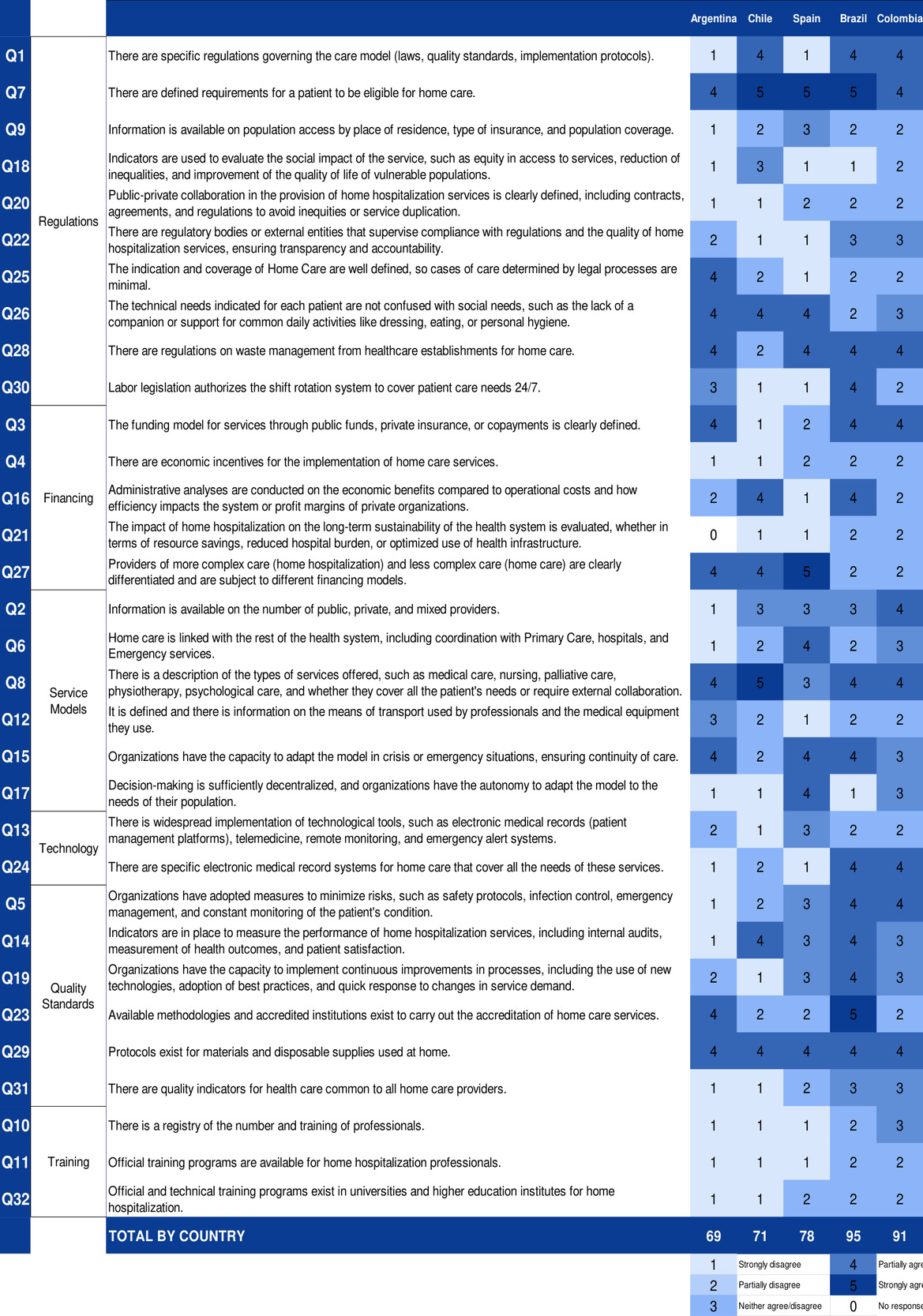
A cross-sectional survey design was employed to examine key features of advanced home-based care models in Colombia, Brazil, Chile, Argentina, and Spain, collecting responses during November and December 2024. Survey questions (Figure 1) examined a total of 32 criteria organized into 6 categories: regulations (10 criteria), financing (5 criteria), service models (6 criteria), technology (2 criteria), quality standards (6 criteria), and training (3 criteria). Questions were validated by country representatives in a meeting of ASIADES’ scientific committee.
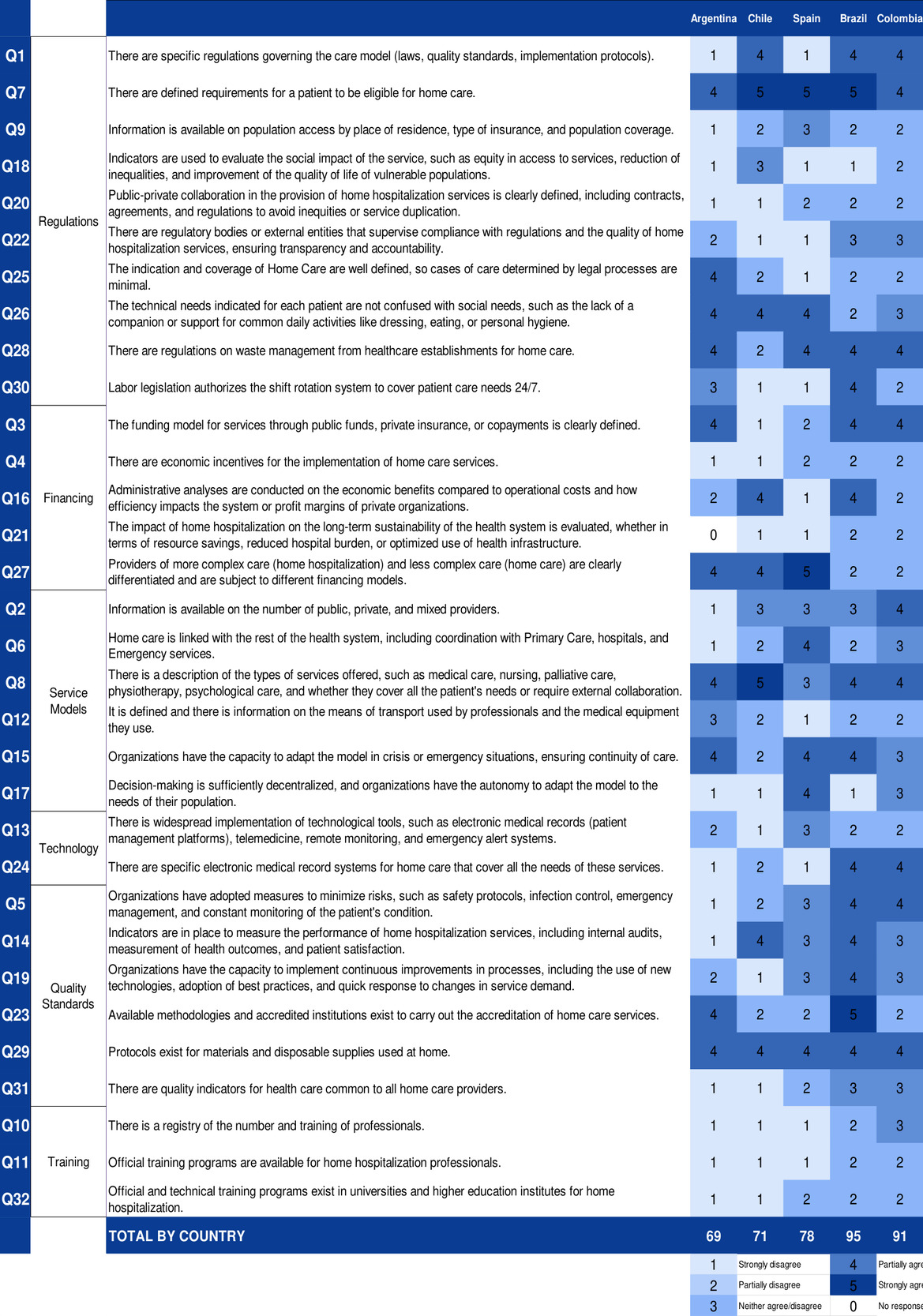
The survey questionnaire was developed collaboratively by members of the ASIADES Scientific Committee, which included representatives from all five participating countries. Each country designated at least one expert who contributed to the question design process, ensuring balanced geographic input. Draft versions of the instrument were circulated among committee members through iterative rounds of discussion and refinement. In cases of disagreement regarding question wording or content, consensus was reached through group deliberation, with priority given to clarity, cross-country applicability, and regulatory relevance. This iterative process continued until unanimous agreement was reached. Responses were rated on a 5-point Likert scale (Likert, 1932) ranging from 1 (strongly disagree) to 5 (strongly agree), with higher scores reflecting traits considered favorable in the context of home-based care.
Participants to answer the survey were selected through the national networks of the Ibero-American Association of Home Health Care (ASIADES). In each country, 3 to 5 senior professionals with recognized expertise in advanced home medicine (Hospital at Home / Home Care) were invited to participate. Respondents included medical directors, executive managers, and presidents of national associations, all of whom hold senior leadership positions within hospital-affiliated services or within private home health care organizations.
The number of participants per country was as follows: Brazil (4), Colombia (5), Argentina (4), Chile (3), and Spain (3). To ensure consistency of responses, a national coordinator was identified in each country (a recognized representative of ASIADES), who consolidated the responses of participants when minor divergences occurred, aiming to reflect the majority view.
Although the number of respondents per country varied slightly, they were selected to represent the largest providers and/or national associations in each setting, ensuring that the perspectives captured reflected the most relevant organizations in terms of patient volume, geographical coverage, and regulatory engagement. This approach prioritized expert consensus from national leaders rather than a population-based sample, which would not be feasible given the heterogeneity of providers across Ibero-America.
Data collection
Data was collected using an online questionnaire distributed via the Google Forms platform, an online survey tool by Google®. A link was shared with respondents to give access to the survey, and responses were stored and managed electronically. Of the five national representatives, all responded to every question except for one representative who did not answer one question.
Data analysis
Quantitative data was statistically analyzed to organize and interpret respondents’ answers. Descriptive statistics, including mean scores, medians, and interquartile ranges (calculated using Python version 3.13.0 and the NumPy library version 2.2.6), were calculated to capture the overall trends in each country, and cross-country comparisons were conducted on thematically related groups of questions from each of the 6 categories, enabling the understanding and highlighting differences in how each aspect of the healthcare model is represented in each country. Given the ordinal nature of the data and the small sample size per country, a non-parametric Kruskal–Wallis H test was used to assess whether the observed differences across countries were statistically significant (α = 0.05). This test was selected due to its suitability for comparing medians among multiple independent groups when normality and homogeneity of variances cannot be assumed (calculated using Python version 3.13.0 and the SciPy library version 1.15.3).
Ethics/Considerations
This study was conducted as a voluntary evaluation survey among professionals working in advanced home healthcare. No personal, identifiable, or sensitive data were collected, and participation implied consent through completion and submission of the questionnaire. In accordance with established ethical standards for minimal-risk evaluative studies, the requirement for formal ethics committee review was collectively re-evaluated by all survey respondents and by ASIADES (Ibero-American Association of Home Healthcare). After careful consideration, the group reaffirmed that formal submission was not necessary, given the study’s evaluative nature, absence of identifiable data, and previously demonstrated ethical soundness of the research procedures.
Results
Overall National Agreement
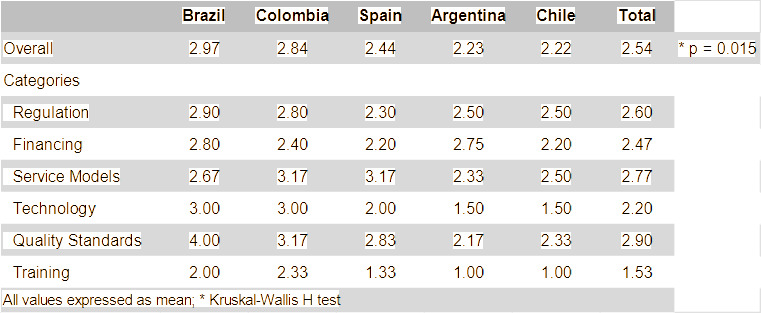
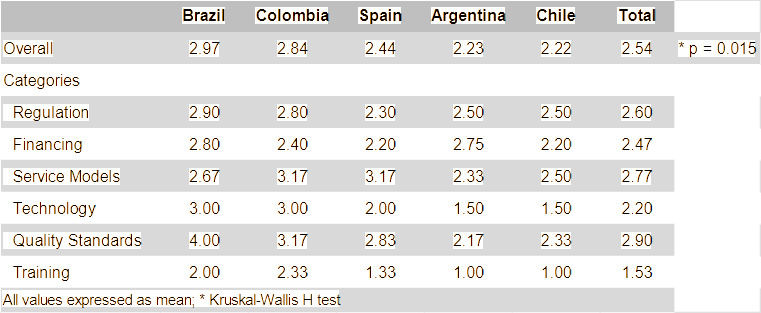
Data was collected during November and December 2024. At the end of the data collection, responses were analyzed both as a whole and within specific categories (Figure 1). Overall, Brazil (mean value M of 2.97, median = 3, IQR = 2.0) and Colombia (M = 2.84, median = 3, IQR = 2.0) demonstrated a higher general level of agreement than Spain (M = 2.44, median = 2, IQR = 2.25), Argentina (M = 2.23, median = 2, IQR = 3.0), and Chile (M = 2.22, median = 2, IQR = 2.25). When aggregating responses across all countries, the average collective agreement was 2.54. A Kruskal-Wallis H test was performed on this data and revealed that the differences observed were statistically significant (H (4) = 12.326, p = .015) (Figure 2).
Quality Standards and Service Models
In general, the categories Quality Standards (M = 2.90) and Service Models (M = 2.77) showcased the highest international agreement (Figure 1). Notably, Brazil reported the highest level of agreement in the Quality Standards category (M = 4.00), whereas Colombia and Spain held the highest scores in the Service Models category (M = 3.17) (Figure 2). However, despite the Quality Standards and Service Models categories demonstrating high levels of agreement, a question specifically related to quality indicators received lower scores from all participating countries (see question Q31 on Figure 1).
Regulation
With respect to Regulation (M = 2.60), scores varied significantly between countries on questions related to regulatory clarity and standardized regulatory frameworks, while lower scores were given on questions about public-private coordination and equity in access. Higher agreement was observed on the subject of eligibility criteria (See questions Q1, Q7, Q18, Q20, Q22, Q25, and Q28 on Figure 1).
Financing
The Financing domain (M = 2.47) showed low levels of agreement across countries regarding funding mechanisms and sustainability of advanced home care. Responses indicated limited definition of public or private reimbursement models, scarce economic incentives for service implementation (See questions Q3 and Q4 on Figure1), and inconsistent evaluation of cost-effectiveness or long-term sustainability. Differentiation between financing models for higher- and lower-complexity care also varied notably among countries (See questions Q16, Q21 and Q27 on Figure 1).
Technology and Training
Finally, the Training category exhibited the lowest level of agreement (M = 1.53), followed by Technology (M = 2.20) (Figure 2). Questions relating to the use of electronic medical records, telemedicine, and remote monitoring received low scores from some respondents (see questions Q13 and Q24 on Figure 1). However, greater variability in responses was observed in the Technology category compared to Training.
Discussion
The findings of this study highlight significant heterogeneity in the implementation of advanced home care models across the analyzed Ibero-American countries. While common elements such as defined eligibility criteria and a general orientation towards quality-centered models are present, marked differences exist, particularly in regulation, financing, technological adoption, and staff training.
A consistent pattern in the data is the high variation of care models and quality standards, with Brazil standing out in the latter aspect and Colombia and Spain showing the best performance in service model design. The findings of this study align with existing literature that underscores the variability and challenges in implementing advanced home care models across different regions.9 Notably, disparities in training requirements and regulatory frameworks have been identified as significant factors influencing the quality of care.
Technological and training dimensions were systematically the worst evaluated, evidencing shared structural weaknesses. The low adoption of technologies such as electronic health records, telemedicine, or remote monitoring reinforces the idea that digital advances in advanced home care are not institutionalized but have occurred reactively, for example, in response to health crises like COVID-19. A recent systematic review of telemedicine in Latin America identified persistent barriers, with the pandemic accelerating but not consolidating digital adoption.10,11
Insufficient training of health personnel remains a critical gap in advanced home care. This aligns with international evidence showing a general lack of structured programs for home-based care,12 and with U.S. studies demonstrating that home care aides—despite their frontline role—are often undervalued, excluded from team-based models, and limited by inconsistent delegation laws and inadequate training.13 These findings underscore the need for comprehensive workforce strategies that integrate all tiers of home-care staff and adopt person-centered educational approaches. Recent research confirms that specialized training is essential for the safety and effectiveness of Hospital at Home programs.14,15
Comparatively, Brazil and Colombia scored highest, likely reflecting more consistent public policies, stronger integration across levels of care, and clearer incentives for sector growth.16 In Brazil, the rapid expansion of home care and more defined national frameworks have supported service consolidation and broader coverage. In contrast, Spain, Argentina, and Chile showed lower scores, possibly due to less standardized regulations and weaker public-private coordination. Although Spain has a pioneering role and one of the region’s most structured national guidelines (SEHAD), implementation varies across regions, which may explain its comparatively lower performance. This variability highlights the need for regional platforms such as ASIADES to support the dissemination and adaptation of best practices. Such regional platforms are intended to support knowledge sharing and local adaptation, rather than replace national or subnational regulatory frameworks.
Furthermore, the evaluation of the normative dimension reflects regulatory heterogeneity. Studies have indicated that the lack of effective integration of health service networks and the absence of solid regulatory frameworks hinder coordination and continuity of care, essential aspects for quality in advanced home care.17,18
Implications for public policy and practice
The findings of this study highlight persistent disparities and structural gaps that require coordinated regional action. Health authorities should prioritize the creation and enforcement of clear regulatory frameworks defining scope, quality standards, and operational criteria for advanced home-based care. The lack of regulatory clarity in several countries compromises service consistency and safety; shared regional guidelines—supported by organizations such as ASIADES—could promote alignment and mutual learning. Spain’s national guideline for Hospital at Home, developed by SEHAD, provides a structured reference model that could inform similar efforts across the region.19,20
Improving equity in access to advanced home care also demands addressing resource limitations and uneven digital infrastructure. As telemonitoring and virtual consultations are essential components of safe and scalable home-based care, investments in digital health, broadband expansion, and incentives for workforce distribution in remote areas are critical. This aligns with WHO recommendations that emphasize digital inclusion as a pillar of universal health coverage.21
Another priority is strengthening professional training. The absence of formal education programs in advanced home-based care mirrors global evidence that workforce preparation directly affects care quality and safety.16 Governments and academic institutions should institutionalize national curricula covering advanced home care competencies, geriatrics, palliative care, and digital tools.
Finally, concerns about financial sustainability underscore the need to revise current funding models. Advanced home care should be positioned not only as a cost-saving alternative but as a fully supported care modality. Evidence from Brazil demonstrates that structured home-based programs can reduce readmissions and be cost-effective, especially when aligned with private sector incentives.22 Innovative financing mechanisms—such as bundled payments and value-based reimbursement—may help provide stable, long-term support for the expansion of home-based care.
The study has limitations that may affect its interpretation. First, the small sample size (3–5 experts per country) limits generalizability, reduces representativeness, and restricts statistical power; larger samples would better reflect within-country diversity and allow more robust subgroup analyses. Although the study offers valuable national-level insights, findings may not fully apply to subnational or rural settings. In addition, the scale and maturity of Hospital at Home programs vary markedly across countries, which may have influenced responses, since similar numbers of experts were consulted despite differences in program prevalence. Future research should account for program scale to better contextualize cross-country comparisons.
Second, the aggregated national responses based on consensus might obscure intra-country variation, not reflecting regional differences in policy implementation or service availability.
Third, the use of a Likert scale can limit the depth of insights gathered, meaning data may not fully capture the nuances of regulatory frameworks, institutional capacities, or service delivery models.
In addition, the risk of self-reporting bias should be considered. Respondents might overestimate the strengths of their national models or align their responses with perceived expectations. Social desirability bias is particularly relevant in surveys involving senior stakeholders with vested interests in policy outcomes.
Proposed action or practical recommendations
Based on the study’s findings, several practical actions can strengthen advanced home care across Ibero-America. Regional organizations such as ASIADES should lead the creation of shared regulatory, training, digital, and quality standards to harmonize national models while respecting local contexts. ASIADES could also coordinate a regional observatory or data-sharing platform to benchmark performance and promote continuous improvement.
Knowledge exchange should be supported through structured cooperation mechanisms—such as bilateral technical support, regional forums, and professional fellowships—enabling countries to learn from successful models. Collaboration with governments, academic institutions, and civil society is essential to build workforce capacity, modernize regulation and funding, and ensure equitable access to digital tools.
Aligning these initiatives with global frameworks, including WHO’s Digital Health Strategy and Universal Health Coverage, may further attract international support and position the region as a contributor to global advances in home-based care.
Conclusion
This study highlights significant variability in the development and implementation of advanced home care models across Ibero-American countries. While Brazil and Colombia show comparatively stronger regulatory and service frameworks, widespread gaps persist in workforce training, digital health integration, and consistent regulatory standards. The absence of unified frameworks and formal capacity-building programs limits the scalability, quality, and equity of home-based care services in the region.
To address these challenges, coordinated regional efforts are needed to define common standards, foster institutional collaboration, and promote digital transformation. Organizations such as ASIADES are well-positioned to lead initiatives in benchmarking, capacity-building, and cross-national knowledge exchange. Strengthening advanced home care as an integral component of health systems will require joint action from policymakers, academic institutions, and care providers to ensure access, quality, and sustainability.
Conflict of Interest Disclosures
All authors declare that they have no conflicts of interest related to this article. No financial relationships, activities, or affiliations influenced the conduct, analysis, or reporting of this study.
Data sharing statement
Deidentified data that support the findings of this study, along with the data collection instrument, are available from the corresponding author upon reasonable request. Data will be shared with qualified investigators for research purposes after approval of a methodologically sound proposal. No additional, unpublished data from this study are available.
Author Contributions
Claudio Flauzino Oliveira and Manuel Mirón-Rubio had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: Cláudio Flauzino de Oliveira, Manuel Mirón-Rubio, Federico Sierra, Adrián Fernández, Adriana Patricia Forero-Hincapie, Sonia Lucía Arias, Loreto Yañez.
Acquisition, analysis, or interpretation of data: Cláudio Flauzino de Oliveira, Manuel Mirón-Rubio, Federico Sierra, Pablo Bertrand, Adrián Fernández, Adriana Patricia Forero-Hincapie, Sonia Lucía Arias, Loreto Yañez, Víctor González-Ramallo, Olga Lucía Pinzón Espitia, Diogo Scordamaglia de Oliveira, Heloísa Gaspar
Drafting of the manuscript: Cláudio Flauzino de Oliveira, Manuel Mirón-Rubio, Diogo Scordamaglia de Oliveira, Heloísa Gaspar
Critical revision of the manuscript for important intellectual content: Cláudio Flauzino de Oliveira, Manuel Mirón-Rubio, Adrián Fernández, Olga Lucía Pinzón Espitia, Heloísa Gaspar
Statistical analysis: Cláudio Flauzino de Oliveira, Diogo Scordamaglia de Oliveira
Administrative, technical, or material support: Sonia Lucía Arias
Study supervision: Cláudio Flauzino de Oliveira, Manuel Mirón-Rubio