Key points
Question
What factors enable or hinder the successful implementation of Hospital at Home (HaH) services in England, particularly in response to NHS England’s 2021 policy promoting ‘virtual wards’?
Findings
Five key themes influenced HaH implementation across eight services and three Integrated Care Systems:
-
Adaptation of clinical practice: Success required clinicians to modify care processes, electronic records use, and interdisciplinary roles for home-based settings.
-
Change agents and leadership: Effective leadership and prior experience in innovation were critical for overcoming implementation challenges.
-
Access to resources and support: Funding, technology, staffing, and senior managerial support enabled service growth, though inconsistent access created barriers.
-
Governance structures: Supportive, flexible governance enabled innovation, while rigid or unclear policies led to service tensions and delays.
-
Shared learning and stakeholder engagement: Collaboration within MDTs and ongoing dialogue with hospital-based clinicians helped integrate and expand HaH pathways.
Meaning
To scale HaH services effectively, health systems must invest in adaptive clinical practices, distributed leadership, flexible governance, and structured learning environments. Policymakers should recognize HaH as a complex innovation that requires time, resources, and context-sensitive approaches to embed and sustain. Early funding helped, but long-term scale-up needs systemic support beyond initial implementation.
Introduction
Hospital at Home delivers acute care in the patient’s usual place of residence. There is growing evidence of its efficacy, primarily focused on clinical and cost effectiveness.1 In 2022 the world Hospital at Home community released research priorities for HaH, including the identification of enablers and barriers for implementation and scaling of services.2
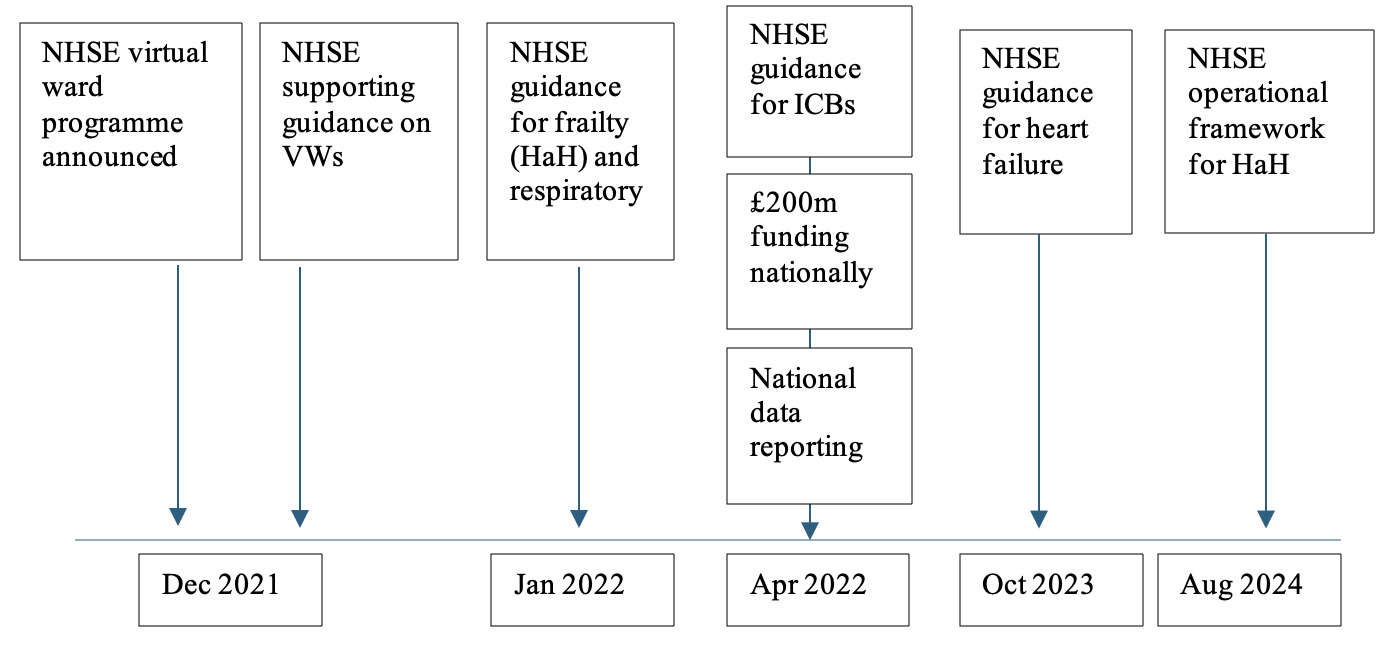
In 2021 NHS England (NHSE) implemented a policy encouraging all Integrated Care Systems (ICSs) to establish ‘virtual ward’ services,3 however little is known about the factors at service level and the wider context that influences implementation. Virtual Wards were initially conceived as a technology-supported remote monitoring system,4 rather than delivering acute multidisciplinary care at home. However, the NHS England 2024 operational framework has renamed these services ‘Hospital at Home’ and changed the specification so that the care model is closer to the internationally recognised HaH definition.5 This change of emphasis, provides a unique opportunity to study the implementation of services at a various of stages of maturity (see Figure 1).

A 2024 Cochrane review found 52 qualitative studies in the literature on barriers and facilitators of HaH services, identifying four main themes6: development of stakeholder relationships; processes, resources and skills required for implementation; acceptability and caregiver impacts; and sustainability of services. It was noted that all studies had methodological concerns, and that 16 were subacute or rehabilitation-based care which would not meet the world Hospital at Home definition.7 Furthermore, the review noted a lack of evidence at a healthcare system level (i.e. at an organisational level above that of direct care providers), mostly being individual services reviews, and none were carried out in response to the reform of a national healthcare management body – the main mechanism through which large scale future HaH programmes are likely to be delivered.
In order to fill the gap outline by the Cochrane review we set out to study system level (through the ICBs) and provider level (through individual sites) of HaH. This study seeks to understand the service and system-level factors influencing the implementation of HaH services in response to NHS England’s virtual ward policy
Methods
We used a comparative qualitative case study design, which is a methodology for studying health policy implementation and change practices within real world contexts.
Our case studies comprised eight HaH services (described as services in this paper) across three integrated care systems (described as systems in this paper) which reflected inner city and more rural geographies (see supplemental information for details). An ICS is a local health partnership in England consisting of health and social care providers and commissioners responsible for NHSE policy implement. Sites were selected to provide diversity and complexity of context comparison8 and to understand how different system and service contexts and organising processes influence implementing ‘virtual ward’ and HaH services. We used multiple approaches to data collection, including observations of everyday activities, interviews and documentary sources, in accordance with established qualitative research techniques.9
Semi structured interviews10 were undertaken with 81 participants including clinicians (medics, nurses and allied health professionals), policy makers and managers (see Table 1) between 2023-2024. Participants were initially purposively sampled then ‘snowball’ sampling was used to identify additional participants. Participants provided written consent to take part in this study. A topic guide was developed and subsequently refined to sensitise it to arising themes. Interviews were audio recorded and transcribed. We undertook observation for all services, including site visits, referral processes, multidisciplinary team (MDT) meetings, documentation and clinical care processes. Observations were recorded through detailed notes that were written up, in full, within 24 hours.11 Documents collected included national and local policies, service standard operating procedures (SOPs) and patient feedback.
A thematic analysis12 of our data progressed through three partially overlapping stages, involving: i) data coding; ii) theme identification and; iii) theme refinement and definition. Coding was performed independently by 2 of the researchers to identify initial themes, then discussed and refined by the wider research team. A rigorous approach was employed through continuous triangulation across our multiple data sources (i.e. interviews, documents and observations) and searching for repeated occurrences and/or absences of events and categories, across places, times, people and situations.9,13 Participant feedback on themes was sought through a workshop at the end of the data collection.
Ethics approval was granted through the University Warwick (ethics committee approval reference number: HSSREC 61/22-23)
Findings
The services included in our study covered a range of clinical specialties including frailty, respiratory, paediatrics, palliative care and general surgery. Sites provided three main models of care: face to face HaH; hybrid face to face combined with remote monitoring; and remote monitoring only with reliance on other teams or hospital admission for face to face review. All sites were consistent with the NHSE 2021 operational policy guidance,4 although services represented a variety of service configurations and levels of care which is consistent with other studies14
We found five main themes that impacted implementation (see Table 2): clinical practice adaptions; change agents and leadership; access to resource and support; governance; shared learning and dialogue with clinical stakeholders.
Clinical practice adaptions
Implementation of HaH services were enabled where MDTs were open to adapting clinical practices to support acute care delivery in home settings. This involved innovating new care models through a complex range of change management activities that simultaneously supported delivering acute care in a geographically dispersed way and accommodating multiprofessional practice standards. We have grouped these into three domains which relate to the professional standards common to healthcare professionals: clinical care process; electronic patient records (EPR) and documentation; and interdisciplinarity.
Clinical care processes – successful adaptation
Clinical care processes, defined as the way of delivering care, were often different or outside the traditional scope of the professional. Clinicians able to improvise and adapt their clinical practice to the home setting, found it easier to deliver care e.g. by modifying processes to undertake clinical examinations or observations, or using remote monitoring or video calls. Clinicians described adapting to the challenges of delivering care, where the equipment may not be set up for clinical assessment. In order to undertake an ultrasound one clinician needed to remove the arm of the chair the patient was seated in to have sufficient access, another clinician described using a head torch to increase the light for placing venous access devices (see Table 3) and others utilised household items such as picture hooks or a lamp to replace a drip stand.
Clinical care processes – challenges to adaptation
Where services were unable to adapt their clinical practice, either due to perceived risk or objection to the clinical model, they relied on a traditional hospital based approach to deliver care. This included bringing patients into the hospital for physical assessments or to receive medications deemed too risky to be administered at home (see Table 3).
Electronic Patient Records (EPR) and Documentation – successful adaptation
There are no current standards for EPR within HaH in the NHS and in particular there are no recommendations to avoid duplication of recording. New technologies or ways of documenting care were embraced to ensure services maintained their governance standards. Successful services worked to overcome challenges with existing EPR systems ensuring suitability for use by community and hospital based clinicians. One service had worked closely with their IT department to produce a version of their EPR that could be used on a tablet or smartphone so that clinicians in the home could input directly into it, and hospital based clinicians could view their documentation remotely.
Electronic Patient Records (EPR) and Documentation – challenges to adaptation
Even with some modifications to their patient records systems, duplication was observed across multiple systems. One service was required to document on a community and hospital based EPR system, and on their remote monitoring platform. Information could not easily be extracted for reporting requirements which resulted in further duplication of recording to support mandated reporting by NHS England. Where these challenges were not successfully addressed, one service had to stop treating patients until a resolution could be found (see Table 3).
Interdisciplinarity – successful adaptation
MDTs typically included a range of physcians, nurses and allied health professionals. We found that the roles of clinicians within the MDT were modified so services could work efficiently. Clinicians described taking on roles that would not traditionally be in the scope of their profession. For example a consultant medic described assisting a nursing colleague with a patient’s personal hygiene during a visit (see Table 3). Shared clinical leadership and responsibility for patients across the full MDT was commonly seen. Trust was placed in the visiting clinicians by senior decision makers. These multidisciplinary relationships supported shared learning and collective innovation within services.
Interdisciplinarity – challenges to adaptation
Implementation was impeded when MDT members were averse to adapting practices to support interdisciplinarity. For example, where services did not have the provision for medical review at home we observed sustained disagreements in MDTs around the clinical responsibilities for patient care. In these settings, clinicians repeatedly sited lack of confidence in a model where a consultant was not physically seeing the patient but was still held legally responsible for care delivery.
Change agents and clinical leadership
Leaders of hospital at home services came from a variety of clinical backgrounds. Where implementation was more established or progressing more rapidly, leaders and/or change agents had prior experience of developing new services or adapting their professional practices to new clinical practice environments . This was not always within acute care or HaH services. These leaders were able to draw on previous experiences to navigate challenges in the implementation processes. They also described a clear vision of the service they were trying to achieve, and were willing to be flexible in their approach.
Governance
Governance structures varied between systems and we found examples of multi-provider collaboratives, system wide steering groups and ad hoc support. These arrangements tended to focus on operational or financial performance of services at a system level. Governance systems struggled to understand the variation in models and often focused on encouraging standardisation of practice across geographical areas. This led to tensions between systems and services around assessments of operational performance (see Table 3). Where system support was more ad hoc, services felt they had more freedom to provide services in a model suited to their local needs and resources. Mostly system level implementation support and governance were subsumed into existing managerial roles.
Although NHSE provided policy guidance to support governance structures, the policy documents were changed during the period of this study. While policy makers and most system managers stated they found the guidance to be clear, clinicians found multiple ways to interpret the guidance to ensure they met the required standards, as evidenced by the variety of service models encountered within this study.
Access to resource and support
Access to resources and support were essential for services to progress their programme. We have divided this into three domains: centralised funding; technology; and staffing and senior support.
Centralised funding
The NHS England two year funding programme was widely viewed as facilitating service implementation. Centralised funding supported service providers to recruit staff, expand teams and introduce technological and clinical developments, allowing services to grow and establish in a short timeframe. However in some situations the flow of money from systems to services was complex (see Table 3). Services experienced challenges with the temporary nature of some funding leading to problems with staff recruitment or training to the appropriate level. Despite funding being available, some services reported difficulty in recruiting suitably qualified staff due to the number of services being set up simultaneously. Difficulties also occurred within systems containing multiple hospital trusts and one service had to stop a specific pathway due to funding disagreements between acute and community providers. When the two-year funding programme ended some services reduced bed capacity within their HaH programmes to meet new budgetary requirements.
Technology
Some services were readily able to access remote patient monitoring technologies through system wide schemes, thereby allowing more rapid implementation into their HaH programme. In one system a region-wide remote patient monitoring solution had been procured for all services. Support was also provided with the technology implementation and refining it to suit the local need. Conversely services within this region reported challenges in accessing other technologies, such as point of care testing, as the system had no further budget to support these. Other systems found the region wide procurement opportunities difficult and were unable to agree with other service providers on the specifications required or struggled to find equipment that met their needs (see Table 3).
Access to staffing and senior support
The multidisciplinary team was central to the delivery of all models of HaH care. Access to appropriately trained staff was crucial for all services to increase their capacity. In one system, to overcome recruitment challenges, nursing had been outsourced to a third party provider. This arrangement was an enabler by facilitating nursing staff to deliver care to patients who lived outside this service’s usual geographical service boundaries.
Leaders described support and encouragement from senior management as being important for service development. Services with senior support found it easier to progress innovation and adaption of clinical policy and practice through complex hospital-based committees and governance processes. Where senior managers supported HaH care, this increased access to funding and technologies described above (see Table 3).
Shared learning and dialogue with clinical stakeholders
We found that implementation was supported where services and systems could support HaH MDTs learning to develop new care pathways and service models together. Shared learning systems were also required to help professional service users (e.g. other clinical colleagues working in acute care and community specialties) understand how to make use of these new services for their patient populations. We have organised this section into two domains: shared learning arrangements for the MDT: and clinical engagement and dialogue with clinical stakeholders and service users
Shared learning for the MDT
At service level, individuals created opportunities to learn from each other, e.g. accessing expertise from more established sites through site visits, and established professional interest groups sharing learning together. Clinicians described supporting learning within the MDT as a key role in HaH. One clinician described supporting a range of MDT members to learn to use point-of-care ultrasound, a task previously limited to medical staff.
Systems were keen to support shared learning and we found a variety of activities including events and meetings to share learning internally. One system was supporting provider development sessions, where services could feed back on new pathways being developed and have an opportunity to share learning, although clinical attendance at these was variable. For wider collaboration, systems relied heavily on the NHS Futures platform which had a range of webinars during the early stages of policy implementation and a platform for sharing documents. Sharing of knowledge through the implementation stage was not usually clinically led and was mostly ad hoc.
Dialogue with clinical stakeholders
Clinicians described needing to maintain an ongoing dialogue with their hospital-based colleagues about their service and newly developed pathways of care. This increased confidence in referrals to the HaH pathways and helped to bring patients into the service. Furthermore this dialogue reduced isolated of clinicians from their hospital based colleagues while adapting clinical practices for home based care.
Leaders developed relationships with key stakeholders and were persuasive when they met resistance to their implementation goals. A service leader described meeting regularly with consultants and specialist nurses from a specific specialty to allay fears that the HaH service was taking over their roles. They described changing their conversational style depending on who they were talking to and ultimately bringing them into the service where they now work together to support patients jointly.
Service implementation was impeded when service leaders had difficulties engaging clinical specialties and building relationships to overcome colleague concerns. Several services described ambitions to develop new care pathways being prevented by concerns from clinical colleagues about increasing workload and perceptions of increased risks (see Table 3).
Discussion
We believe that this is the first study in England to look at the barriers and facilitators to implementation of HaH services and adds to a relatively small evidence base globally. Although there have been some studies looking at early support discharge programmes,6 this study is unique and extends the extant evidence base in a number of ways. Firstly, our study considers implementation at both a service and system level. Secondly, our research design included input from a wide range of stakeholders including clinicians, managers and policy makers with an extensive range of experience working across the HaH field of practice. Finally, although our study identified some implementation challenges, we found services implemented new HaH models rapidly and in accordance with the NHS England policies that were in operation at the time.
There have been similar studies examining implementation, barriers and facilitators for HaH globally. Studies from the US, Australia and Singapore have examined single services15,16; focused on patient perceptions17 or stakeholders18; or specialised in residential care19 or rehabilitation.20 However, the context for implementation in England was unique, given the large scale, top-down, directive for services to be set up and the entirely publicly funded health system. Despite these differences in health care systems, similar themes such as leadership and senior support, financial sustainability and stakeholder engagement can be seen throughout the global literature.
Based upon the findings discussed, we have categorised the themes into those that predominantly have their effect at a service or system level. We provide recommendations to support implementation and future service scaling, summarised in Table 4, based upon the key themes identified.
System-Level Recommendations
At the system level, consideration should be given to expanding the remit of existing services to include HaH as an integral component of acute care pathways rather than as a standalone or peripheral initiative. Leveraging existing community and intermediate care structures can reduce duplication and enhance continuity, provided there is adequate investment in workforce, digital infrastructure, and governance frameworks to support this expansion. Stakeholders should be engaged early from both clinical and non-clinical backgrounds15 to support broader understanding of HaH.
There is also a need to establish dedicated HaH leadership roles, rather than assigning responsibility to individuals who already hold multiple operational portfolios. Dedicated leadership provides the necessary focus for service design, cross-sector coordination, and performance oversight, while ensuring accountability for quality and safety.21–23
Sustainability further depends on the creation of long-term financial resourcing models to underpin recruitment, training, and scaling of services. Reliance on short-term pilot funding creates instability and undermines workforce confidence. The initial funding provided by NHSE to start the HaH programmes in England, undoubtedly supported implementation, however further research is required to examine how the changing nature of the funding impacts service scale up and sustainability. Recurrent investment through long term commissioning frameworks would enable systems to build capacity, invest in skills and equipment, and evaluate impact over time.
To promote continuous improvement, systems should formalise clinically led learning from the experiences of teams that have established and evolved HaH services. Much of the current learning remains informal and localised, without drawing on long established UK services or those from countries with well-embedded services such as USA or Australia. Establishing structured, system-wide mechanisms such as professional networks, communities of practice, and shared data repositories, can enable consistent knowledge transfer and accelerate collective progress.24,25
Lastly, systems must tolerate initial variation among providers. Given differences in population needs, local infrastructure, and clinical capability, early implementations will inevitably vary in scope and design. Embracing this variation as part of the innovation cycle26 allows systems to learn from diverse approaches, progressively standardising around evidence-informed best practice rather than enforcing premature uniformity.21,27
Service-Level Recommendations
At the service level, the implementation of HaH requires realistic targets and timelines that reflect the complexity of adapting hospital-based practices to the home environment. The transformation involves not only logistical redesign but also significant cultural change across multidisciplinary teams. Allowing sufficient time for workforce adaptation and iterative learning is critical for maintaining safety and engagement.
Each service should appoint leaders with a proven record of change agency, ideally individuals with prior experience in service innovation or practice adaptation. These leaders play a pivotal role in translating vision into practice, aligning diverse stakeholders, and embedding new models of care. It is equally important that such change agents have visible and sustained support from senior management, ensuring that HaH development is recognised as a strategic organisational priority.
To maximise their effectiveness, change agents must have structured access to a range of developmental and professional activities, including:
-
Peer professional mentoring from more experienced HaH implementers both within the NHS and the global HaH community;
-
Interdisciplinary learning collaboratives, organised through professional societies or system-wide networks;
-
Leadership development programmes to strengthen strategic and operational capability;
-
Clinical skills training across the full multidisciplinary team, ensuring all staff are confident and competent in delivering care in the home environment.
These activities foster professional confidence, build shared purpose, and sustain momentum during the challenging early stages of implementation.
Finally, across both service and system levels, there needs to be greater recognition and acknowledgement that HaH services represent a complex service28 innovation and implementation and scale will take a period of time to embed before services reach their full capacity.
Limitations
This study was conducted within the Midlands region of England, but we believe many of the service level findings are generalisable across services within England. A large number of interviews with clinical staff (representing a wide range of professions), managers and policy makers were included. Whilst our study attempted to have representation from a range of geographical areas, we had more services in urban areas and future work may wish to identify more rural services. Further research could characterise the qualities that successful HaH leaders demonstrate, stakeholder perceptions at different stages of implementation and the financial impacts on implementation.
Conclusion
A range of facilitators and barriers for implementing Hospital at Home services were identified at both a service and system level. Services and systems can use the recommendations to support development and evolving service provision.
Funding
This study was funded by NHS England Midland region. This study was supported by the National Institute for Health Research (NIHR) Applied Research Collaboration (ARC) West Midlands, NIHR Community Healthcare HealthTech Research Centre (HRC) and NIHR Oxford Biomedical Research Centre (BRC). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Data Sharing
The data for this study will not be shared, as we do not have permission from the participants or ethics approval to do so.
Conflicts of interest
None
Author Contributions
Data curation: Sophie E. McGlen (Lead), Sarah Woolley (Supporting). Formal Analysis: Sophie E. McGlen (Lead), Sarah Woolley (Equal), Graeme Currie (Supporting), David Aldulaimi (Supporting), Daniel Lasserson (Supporting). Project administration: Sophie E. McGlen (Lead), Sarah Woolley (Supporting). Writing – original draft: Sophie E. McGlen (Lead). Writing – review & editing: Sophie E. McGlen (Equal), Sarah Woolley (Equal), Graeme Currie (Equal), David Aldulaimi (Supporting), Daniel Lasserson (Equal). Investigation: Sophie E. McGlen (Lead). Conceptualization: Sarah Woolley (Equal), Graeme Currie (Equal), Daniel Lasserson (Supporting). Funding acquisition: Sarah Woolley (Equal), Graeme Currie (Equal). Methodology: Sarah Woolley (Supporting). Supervision: Sarah Woolley (Lead).
Corresponding author
Sophie E. McGlen: sophie.mcglen@wbs.ac.uk