Background
In the United States, close to two million older Americans are completely homebound and another 5.5 million have difficulty or need assistance to leave their homes making access to office-based primary care challenging. Home-based primary care (HBPC) is a model of comprehensive, longitudinal medical care delivered by an interdisciplinary team including physicians, nurse practitioners, nurses, social workers and others directly in patients’ homes. It is designed to provide access to primary medical care for homebound persons. HBPC provides medical care traditionally provided in an ambulatory care setting and does not provide personal supportive care services such as assistance with activities of daily living. Only 12% of homebound older Americans receive HBPC.1
While HBPC care is associated with reductions in emergency department and hospital utilization, lower costs, and better care experience,2 it has been largely ignored in the context of Center for Medicare and Medicaid Services (CMS) care quality initiatives, quality improvement (QI), and value-based care.3 To address this gap, researchers with input from clinicians, policy makers, patients, and caregivers developed HBPC-specific quality of care measures and a quality framework for HBPC.4 In 2018, the National Home-Based Primary Care Learning Network (LN) was created to instill a culture of quality and QI in HBPC through trainings and monthly workshops.3,5 The LN now comprises over 100 HBPC US practices.
LN practices have the opportunity to track the change ideas they test via plan-do-study-act cycles on a common QI learning platform. The aim of this study was to inventory change ideas tested by LN practices, categorize them, and develop a driver diagram to inform a conceptual framework of critical functions of HBPC and current quality of care challenges experienced by HBPC practices.
Methods
We collected all change ideas tested in PDSA cycles conducted by LN practices and entered them into the QI learning platform between March 2020 and November 2024. Change ideas were categorized using directive qualitative content analysis6 by the LN leadership team, which informed the development of a driver diagram (DD).
Results
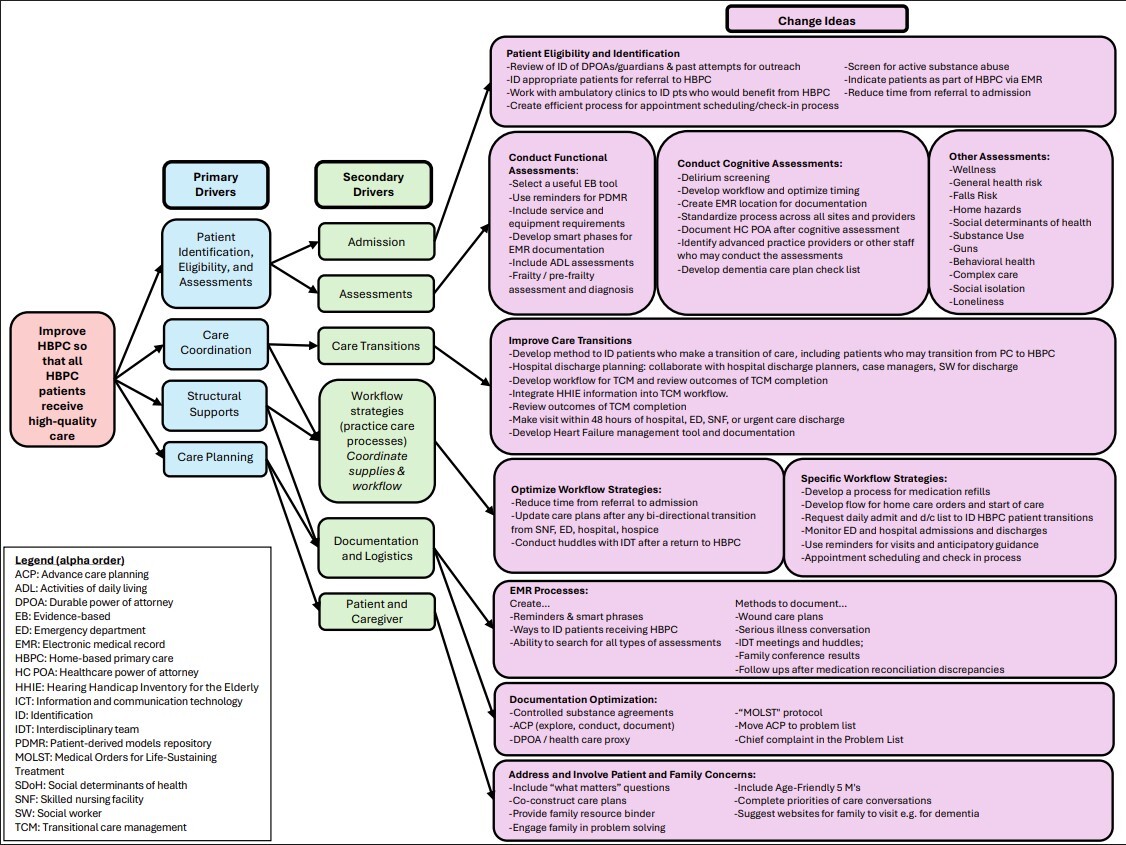
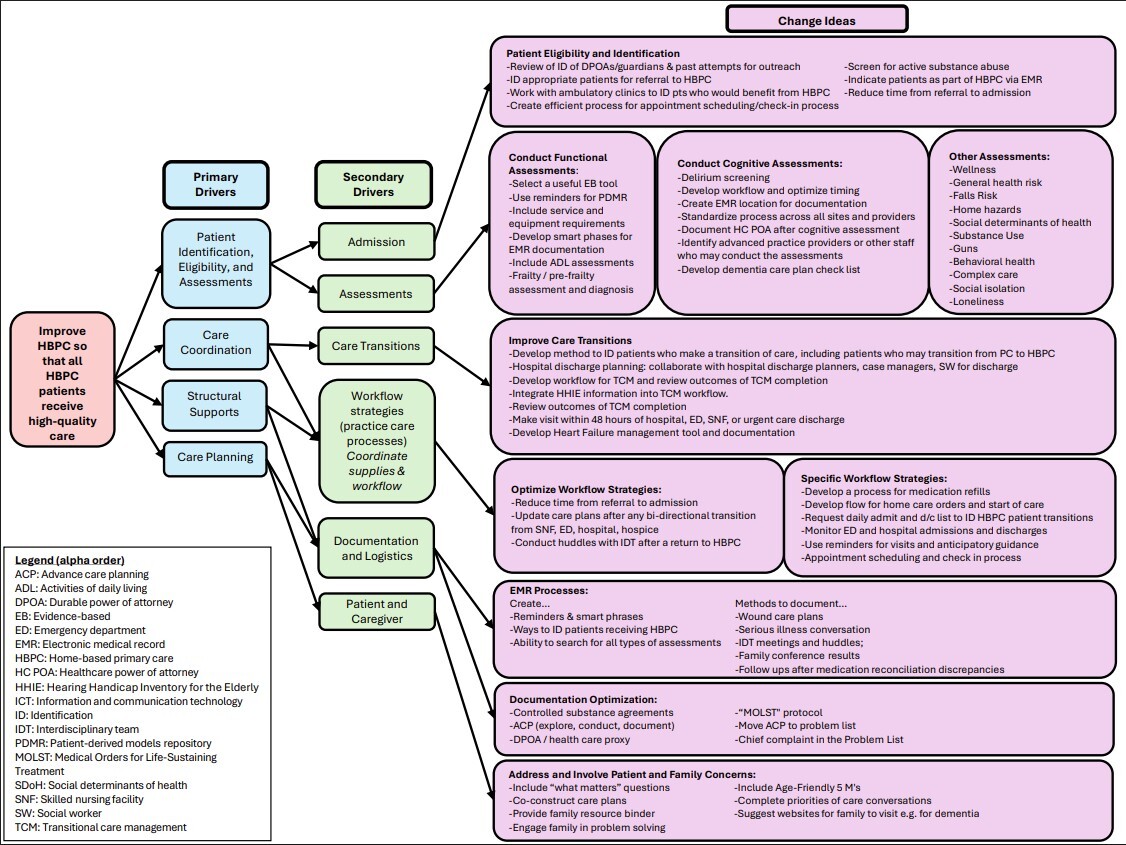
Across 704 PDSA cycles initiated and/or completed by LN practices, 223 unique, non-redundant change ideas were tested. Change ideas were grouped into 10 categories and linked to 6 secondary drivers and 4 primary drivers of change in service of the LN’s aim to improve HBPC so that all HBPC patients receive high-quality HBPC. The 4 primary drivers were: 1) patient identification, eligibility, and assessments; 2) care coordination; 3) care planning; 4) structural supports. Each primary driver links into two secondary drivers reflecting expected overlap in patient care and practice functions. See Figure.
Discussion
Change ideas tested by LN practices reflect the challenges faced by HBPC practices in providing high-quality care to their high-need homebound older adults with high prevalence rates of multimorbidity, functional and cognitive impairment. These conditions require a range of assessments to optimize care. HBPC practices faced challenges effectively addressing these complex needs and sought to improve their ability to: identify and enroll appropriate patients, manage care transitions in a population that has high rates of emergency department and hospital utilization, involve patients and their family caregivers as members of the care team, optimize electronic health record processes for a type of practice for which electronic health records were not designed to accommodate, as well as improve logistics in operating care outside of facility-based office-based primary care.
The main strength of this study is that it provides a wide-ranging description of the quality improvement gaps and care delivery challenges identified by a diverse set of HBPC practices across the US in terms of geographic location, size, staffing models, and profit-status. Main study limitation is overrepresentation of change ideas related to functional and cognitive assessments, which is a product of LN leadership requiring HBPC practices to engage on those topics as their first QI project early in their participation in the LN.
Conclusions
Analysis of change ideas tested in PDSA cycles and the driver diagram from LN QI initiatives provides a useful conceptual framework for HBPC practices to consider in the context of QI to optimize HBPC care delivery. As the LN work continues, we expect these drivers and change ideas to be refined over time. Commitment to QI in HBPC is key to sustainability of the field.
Funding
This work was supported by a grant from The John A. Hartford Foundation a private, nonpartisan, national philanthropy dedicated to improving the care of older adults. The funder had no role in the design, methods, subject recruitment, data collections, analysis and preparation of paper.
COI
Dr. Ritchie Editor for UptoDate (Wolters Kluwer), McGraw Hill, and Oxford University Press.
Dr. Leff is a full-time employee of the Johns Hopkins University School of Medicine and reported receiving personal consulting fees: Chartis Healthcare, the Aligned Health Group, the Kenes Group, and the West Health Institute. Stock options: Member of clinical advisory boards to Honor Care, Dispatch Health, Pager Health. Honoraria: Board of directors of the American Board of Internal Medicine Foundation.
Taylor: no conflicts
Vetter: no conflicts
Sheehan: no conflicts
Kreutzelman: no conflicts
Ethical approval
This work was approved by the institutional review boards of the Johns Hopkins University School of Medicine and MassGeneral Brigham. Protocol #:2020P000693
Data availability
All authors had full access to all of the data. The data are not publicly available.
Acknowledgements
The authors acknowledge the members of the National Home-Based Primary Care Learning Network for the exemplary care they provide their homebound patients.
Author contributions
Michael Vetter: Investigation, formal analysis, project administration, resources, validation, visualization, writing – review & editing
Orla Sheehan: Conceptualization, data curation, investigation, formal analysis, methodology, project administration, validation, visualization, writing – original draft, writing – review & editing
Max Kreutzelman: Data curation, project administration, resources, visualization, writing – review & editing
Christine Ritchie: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, supervision, validation, visualization, writing – original draft, writing – review & editing
Jane Taylor: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, validation, visualization, writing – original draft, writing – review & editing
Bruce Leff: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, supervision, validation, visualization, writing – original draft, writing – review & editing