
KEY POINTS
Question: Which Hospital at Home (HaH) patients are more likely to be escalated back to the brick-and-mortar (BAM) hospital?
Findings: In this retrospective chart review of 1000 HaH patients in an established Canadian adult medical HaH program, advanced cirrhosis, severe heart failure, frailty, metastatic cancer and male gender were significant independent risk factors for escalation. These risk factors were used to create an escalation risk prediction tool.
Meaning: It may be possible to predict an individual patient’s risk of escalation in HaH based upon their risk factors. External validation is required.
INTRODUCTION
Hospital at Home (HaH) is an emerging model of acute care that can be offered to stable patients in lieu of a brick-and-mortar (BAM) hospital admission. In an effort to standardize the global practice of HaH, the Scientific Committee of the World Hospital at Home Congress released its definition of HaH in 2023.1
It is standard practice in HaH to escalate a patient’s care to the BAM hospital if the patient’s condition deteriorates.2 Escalations are an inevitable aspect of HaH by virtue of the patients’ acuity, yet HaH programs aim to limit escalations because they disrupt patient care and are resource intensive. At this point in time, consensus on the optimum escalation rate is lacking, although rates of 6-10% are commonly reported in the literature.3–5
In 2020, the Canadian city of Victoria, British Columbia began an adult HaH program that complies with the WHAHC definition of HaH. The Program operates as an inpatient medical unit of the local tertiary care hospital, providing in-person nursing visits, virtual and in-person physician visits, and 24-hour patient support through the availability of an on-call nurse and physician who can perform home visits after hours. The Patient Eligibility Criteria are listed in Table 1, with different criteria for patients who live with a caregiver and those who live alone. The Program accepts physician referrals for patients who are presently admitted to the hospital. The Program uses intermittent remote vital sign monitoring technology. The Program does not provide soley palliative care because that service is provided by a separate community palliative care program. It does, however, treat patients with a reversible illness who also have an underlying palliative diagnosis such as metastatic cancer.
During the Program’s 4th year of operation, the escalation rate increased unexpectedly from its target of 6-8% to 11.4%. We could not account for the change in the escalation rate, as the eligibility criteria, operating procedures and staff had not changed.
The published literature on escalation risk factors in HaH is limited. Only a few studies have attempted to identify escalation risk factors, and the results have at times been conflicting. For example, two studies that tested the predictive value of a patient’s overall burden of comorbidities (reported as the Charlson Comorbidity Index, which is a composite score of 17 different comorbidities) had opposite findings.6,7 The same two studies also had different results when looking at marital status and escalation risk. They both, however, found that age is not predictive of escalation, but this was contrary to a third study.8 One of the aforementioned studies found a significant correlation between escalation risk and a proprietary mortality risk score that uses a complex algorithm to account for the patient’s admission diagnosis and comorbidities (APR-DRG Risk of Mortality score, 3M Health Information Systems), but it is questionable how useful this risk factor is, given its inaccessibility.6
Seeking to understand why the escalation rate in the Victoria HaH Program had increased by approximately 50%, two subject matter experts (ST, TM) informally reviewed the 37 escalations in the previous six months and noticed a trend: many of the escalated patients had advanced comorbidities that decompensated at home. They did not notice a correlation between escalation and whether a patient lived alone or was of advanced age.
This study aimed to identify which, if any, advanced comorbidities are independently associated with an increased risk of escalation. We hypothesized that certain advanced comorbidities, such as severe heart failure, are significantly associated with escalation. Additionally, we sought to determine whether demographic factors, such as living alone, increase the risk of escalation.
The ultimate goal of our study was to create an easy-to-use tool that predicts the risk of escalation for individual patients. Prediction tools are commonly used in many areas of medicine to assist in clinical decision making, such as the CHADS2 score for predicting stroke risk in atrial fibrillation,9 and the CURB65 score for predicting mortality in pneumonia.10 No such tool for predicting the risk of escalation in HaH exists.
METHODS
Objectives
The primary objective of this analysis was to test the hypothesis that advanced comorbidities of the major organ systems, as well as advanced age, living alone and male gender, are risk factors for escalation in HaH. Provided that escalation risk factors were identified, the secondary objective was to build a clinical prediction tool that provides a patient’s risk of escalation based upon their risk factors.
Population
The study population was the last 1000 consecutive cases in the Victoria HaH Program. All patients in the sample had been an HaH patient at some point during the acute care episode, regardless of whether they were discharged from HaH, or escalated back to the BAM hospital.
Study design
This was a retrospective convenience sample of 1000 consecutive HaH cases over approximately one year. We estimated that a sample of 1000 would be sufficient to generate statistically significant results. We performed a manual review of the hospital electronic medical record, noting the presence or absence of the hypothesized risk factors, which included advanced chronic disease of the major organ systems, frailty, immunosuppression, chemotherapy, advanced age, living alone and male gender. Table 2 lists the 11 hypothesized risk factors, with operational definitions.
We recorded whether the patient had experienced an escalation. We defined escalation as any unplanned transfer of care to the BAM hospital, regardless of whether the patient was transferred back to HaH after the escalation. A planned transfer to the BAM hospital was not classified as an escalation, e.g. for a prearranged surgery. We also noted whether the patient had an unexpected death at home.
To evaluate the risk of escalation associated with each hypothesized risk factor, we created a logistic regression model for the binary event (yes, no) of escalation. All factors were entered simultaneously to adjust for potential confounders, and to assess the independent contribution of each factor to escalation.
In the context of a multivariable logistic regression model, the issue of multiple comparisons is addressed by the model’s estimation of the effect of each factor while adjusting for the effect of the others. This joint estimation accounts for correlations among factors and does not involve separate hypothesis tests for each factor in isolation. Therefore, the model does not require correction methods, such as Bonferroni or False Discovery Rate (FDR), which are typically applied when performing multiple independent tests. Instead, logistic regression provides adjusted estimates and confidence intervals, making it a more appropriate approach for predictive modeling rather than exploratory multiple testing.
We ran two model diagnostics tests: the Hosmer-Lemeshow goodness-of-fit test to assesses whether the observed event rates matched the predicted probabilities, and the Nagelkerke’s R²test to evaluate how well the model explained the outcome.
The multivariable logistic regression model was used to calculate the predicted probability of escalation for every possible combination of risk factors.
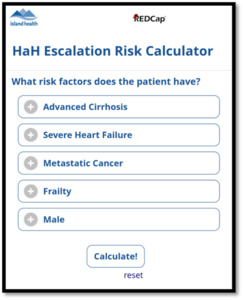
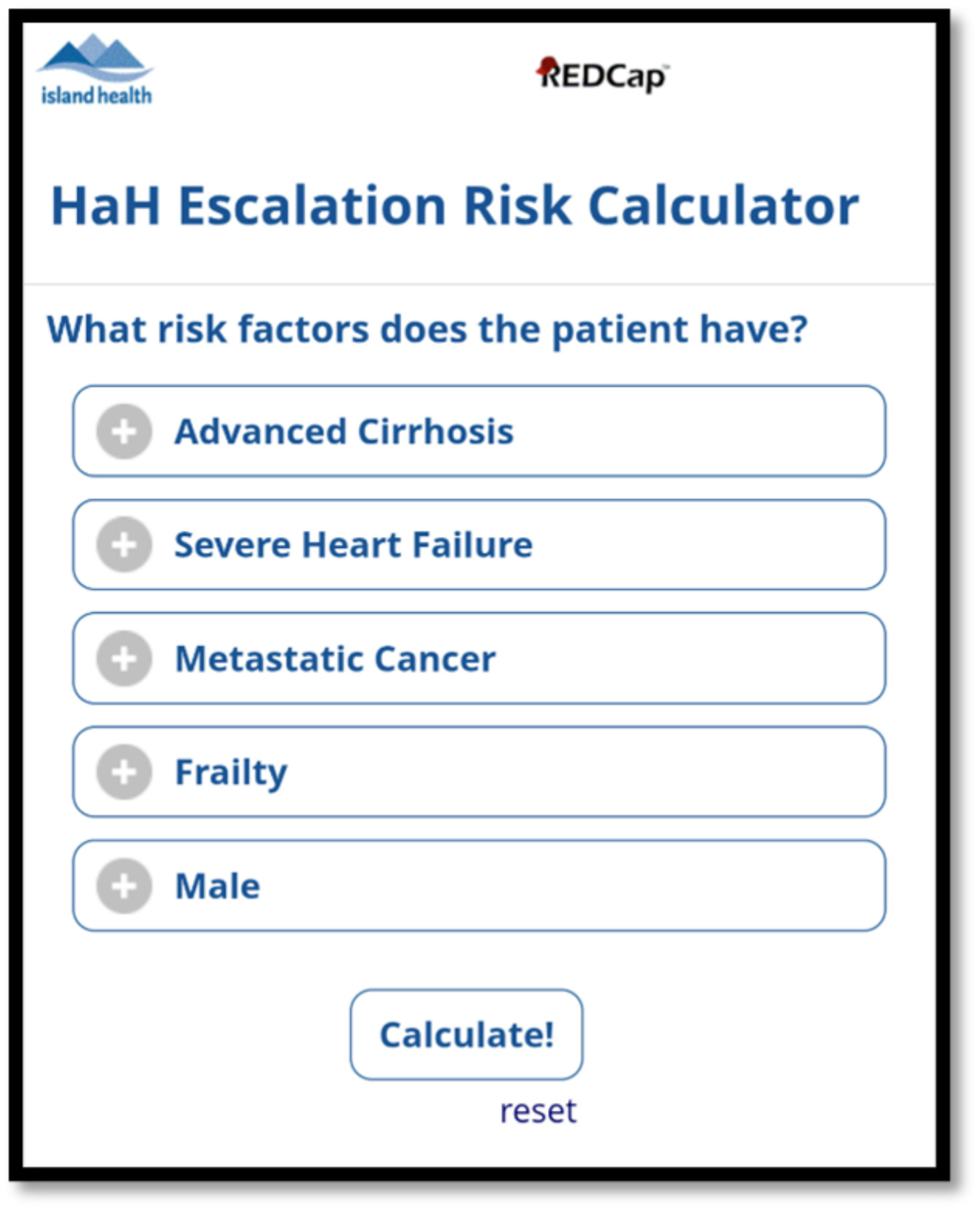
The multivariable logistic regression model also formed the basis of an escalation risk prediction tool. The tool used REDCap Version 14.5.14 as a Web-based calculator to generate an individual patient’s percentage risk of escalation after the user has input the patient’s risk factors.
Data collection and storage
One of the authors (ST) performed the chart review independently. To ensure consistency and reliability, she adhered to an objective definition of each risk factor (Table 2). Records that were incomplete were removed from the analysis. Data were stored in Island Health’s confidential REDCap database.
RESULTS
Of the 1000 cases, 10 records (1%) were incomplete. These records were removed from the analysis, resulting in 990 cases for the study population.
The 990 cases spanned a calendar year, from June 2023 to September 2024. The average patient age was 71, ranging from 17 to 105 years old. The genders were evenly represented (48% men, 52% women). Approximately one quarter of the patients (26%) lived alone. Fifteen percent of patients had been admitted to the Program previously. The average length of stay in the Program was 8.1 days.
Of the 990 cases reviewed, 96 (9.7%) resulted in escalation, and four resulted in an unexpected death at home (0.4%).
The prevalence of each hypothesized risk factor among the 990 cases is shown in Table 3.
The following factors were significantly associated with an increased risk of escalation: advanced cirrhosis, severe heart failure, frailty, metastatic cancer and male gender. As a result, we can conclude that these five factors were escalation risk factors in the study population. The odds ratio (OR) with 95% confidence intervals (CI) and p-value for each escalation risk factor are listed in Table 4.
The Hosmer-Lemeshow test p-value was 0.636, suggesting that our model aligned well with the data. The Nagelkerke’s R² value was 0.047, indicating that the model explained 4.7% of the variability in the outcome. In public health, low R² values are often expected, and models can still be useful for risk prediction even with low R². The focus is more on statistical significance and clinical relevance than on high R² values.
The following hypothesized risk factors were not associated with an increased risk of escalation in the study population and were therefore not escalation risk factors: advanced age, severe renal failure, end stage lung disease, transplant status, chemotherapy and living alone. Their p-values are listed in Table 5.
A patient’s overall risk of escalation for each combination of risk factors is shown in Table 6, with 95% confidence intervals (CI). If a patient had all five risk factors, his risk of escalation was 95%. A patient lacking all risk factors (i.e. a female without severe heart of liver disease, metastatic cancer or frailty) had only a 4.1% risk of escalation.
A patient’s overall risk of escalation, based upon their combination of these five risk factors, can be represented by the logistic regression formula:

with each factor (e.g. [Male], [Metastatic Cancer]) taking the value of 0 or 1 if nonapplicable or applicable, respectively, in that particular patient.
The Web-based escalation risk prediction tool shown in Figure 1 provides an individual patient’s risk of escalation after the user inputs the patient’s risk factors.
DISCUSSION
This study tested the hypothesis that advanced comorbidities of the major organ systems are independent risk factors for escalation in the Victoria HaH Program. We found that certain advanced comorbidities are predictive, whereas others are not. More specifically, advanced cirrhosis, severe heart disease, metastatic cancer and frailty increase the risk of escalation, whereas severe renal failure, end stage lung disease, transplant status, and being on chemotherapy do not. We suspect that the former comorbidities are intrinsically less stable than the latter, and are therefore more likely to decompensate and trigger an escalation back to the BAM hospital.
The different significance of different comorbidities could explain why two studies looking at the relationship between the overall burden of comorbidities and escalation risk had opposite findings.6,7 Our results suggest that a more specific analysis of different comorbidities is required to detect their relevance to escalation risk.
We identified a very high risk of escalation associated with advanced cirrhosis: a medically stable patient with advanced cirrhosis (MELD-Na of 20 or higher) and no other risk factors had a 49.8% risk of escalation. In a study involving a small cohort of patients with cirrhosis who were managed in HaH, Kahn-Boesel et al found that patients with less advanced cirrhosis (median MELD-Na of 12) had an escalation rate of 0%.12 Together, these two studies suggest that HaH is suitable for cirrhosis patients with a maximum MELD-Na score between 12 and 19. As a result of this analysis, the Victoria HaH Program has added advanced cirrhosis to its exclusion criteria. Since the risk of escalation is at least 49.8%, we recommend these patients receive their acute care in the BAM hospital. Should a patient with advanced cirrhosis wish palliation at home, we recommend a referral to our local community palliative care program, as we do not provide purely palliative care.
We also tested the hypotheses that certain demographic factors (advanced age, living alone and gender) increase the risk of escalation. We found that advanced age is not an escalation risk factor, which aligns with the majority of the literature: of the three studies looking at age and escalation risk,6–8 only one found age to be relevant.8
We did not find an association between living alone and escalation, regardless of the patient’s age. To the best of our knowledge, ours is the first study to look at whether the absence of an informal caregiver at home increases the risk of escalation. (Two previous studies reported on marital status, which is not synonymous with caregiver status.6,7)
Lastly, we found that male gender conferred a slightly higher risk of escalation, even in the presence of a caregiver. (The p-value was borderline significant, at 0.057.) This is consistent with the general finding that men have higher mortality rates from chronic conditions than women.13 However, two studies that looked at gender and escalation did not find an association, so our finding is unique and unexplained.6,7
We subsequently created an escalation risk prediction tool for the Victoria HaH Program. This tool has been incorporated into clinical practice in several ways. Firstly, the Program uses the risk prediction tool as part of the consent process, informing potential patients of their likelihood of returning to the BAM hospital unexpectedly. The tool is also used to maintain the target escalation rate of 6-8%: if a patient’s risk of escalation is high, the Program has a goals-of-care conversation with the patient to discuss their wishes in the event of decompensation at home; the Program may decide not to admit a patient with a high risk of escalation who would want escalation in the event of clinical decompensation.
Using the escalation prediction tool to potentially exclude patients with a high risk of escalation may seem ethically problematic, but these exclusions are justified on the basis of patient safety. An escalation puts the escalated patient at risk of harm by delaying care and introducing communication errors. Additionally, escalating a patient is a resource-intensive process that pulls resources away from other HaH patients.
There are several important limitations to our analysis. Firstly, our study did not necessarily identify all escalation risk factors in the study population. We only tested those factors of which we were suspicious. As a result, the percentages generated by our risk prediction tool may be an underestimate of an individual patient’s risk.
Secondly, because our results come from a single site, they may not be generalizable to all HaH programs. For example, by including in-person physician visits, the Victoria Program may have been able to stabilize patients who would have required escalation in a virtual-only program. Similarly, its remote patient monitoring system may have prevented escalations by detecting clinical decompensation earlier. Additional studies are needed to clarify whether different types of HaH programs have different escalation risk factors. A knowledge of how program design relates to escalation risk factors may prove useful in the development of practice standards for HaH.
As another limitation, our study did not include the four unexpected deaths. In retrospect, we believe that an unexpected death should be considered an escalation because an unexpected death is the same clinical phenomenon, namely, a clinical deterioration that cannot be stabilized at home. The unexpected deaths made up only 4% of the escalations in the study population, so we are optimistic that their exclusion did not skew our findings significantly.
Our study was also limited by the small size of the research team: only two subject matter experts proposed the hypothetical risk factors, one assessor performed the chart review, and only one biostatistician was involved in the analysis. The accessor adhered to an objective definition of each hypothesized risk factor (Table 2); however, we did not take any specific measures to ensure consistency and reliability in the chart review process performed by the assessor.
We overlooked the advanced comorbidity of end stage dementia, thereby missing out on the opportunity to comment on whether end stage dementia is a risk factor for escalation. One previous study found that dementia does not increase the risk of escalation.6
Lastly, our study used a convenience sampling approach, which can introduce selection bias. The risk of selection bias was mitigated by the large size of the sample (1000 cases), its representation of an entire calendar year (June 2023 to September 2024) and the fact that the cases were consecutive rather than selected individually.
CONCLUSION
Advanced cirrhosis, severe heart failure, metastatic cancer, frailty and male gender were found to be independent risk factors for escalation in an established Canadian adult medical HaH program that provides in-person and virtual care, after hours support and intermittent vital sign monitoring to patients referred from the hospital. We created a Web-based tool that provides a patient’s overall risk of escalation based upon their risk factors. We encourage other HaH programs to validate our risk factors and our prediction tool, to search for additional risk factors, and to investigate whether different types of HaH programs have different escalation risk factors. Understanding the relationship between escalation risk factors and HaH program design could help inform the standard of care in HaH.
ACKNOWLEDGMENTS
The authors would like to thank Skye Alister Tierney for assisting with data entry, and Arrietty Song for her literature review.
DATA SHARING
The study data can be accessed by contacting the corresponding author.
CONFLICTS OF INTEREST
No relevant disclosures.
AUTHOR CONTRIBUTIONS
Victor Espinosa had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: Dr. Shauna Tierney, Dr. Sean Spina, Victor Espinosa, Tara Mulcaster.
Acquisition, analysis and interpretation of data: Dr. Shauna Tierney, Victor Espinosa, Dr. Sean Spina, Tara Mulcaster
Drafting of the manuscript: Dr. Shauna Tierney
Critical revision of the manuscript for important intellectual content: Dr. Shauna Tierney, Dr. Sean Spina, Victor Espinosa
Statistical analysis: Victor Espinosa
INFORMED CONSENT
Informed consent was not required.
ETHICS APPROVAL
Ethics approval was not required.